Research framework & methods
Image: Making it work, NASHCO Photography (USA)
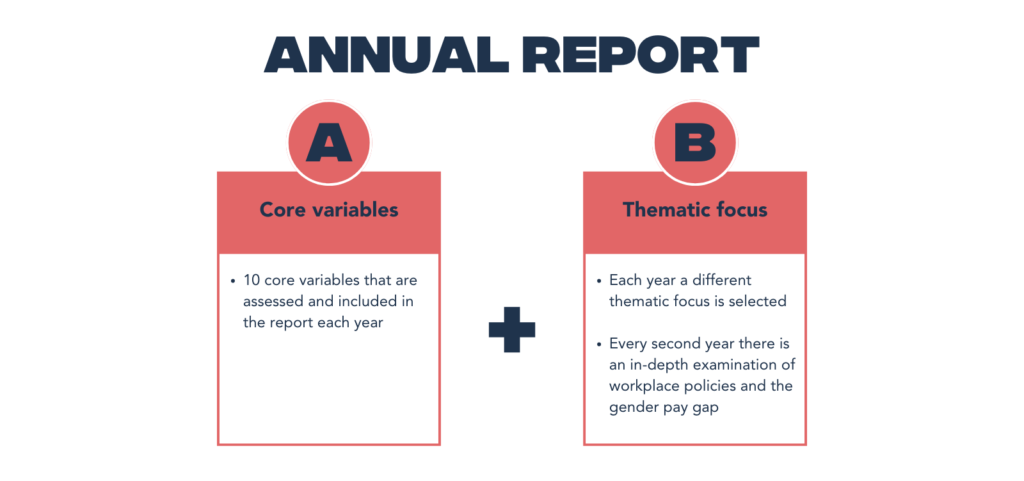
Each year, Global Health 50/50 reviews the gender-related policies and practices of hundreds of global organisations, as published in our Annual Reports and the Gender and Health Index. Since establishing the annual Report and Index in 2018, our research framework and methods have evolved, in response to expanding priorities, the evolving body of global evidence and feedback from assessed organisations. This page presents an overview of the current research framework and the methods used to report on our core variables.
In addition to these core variables, each year we examine a thematic focus and collect organisational data relevant to the theme. The methods used for each thematic focus are often unique and are detailed in the relevant report.
GH5050 core variables
Our variables assess policies and practice across four domains. The detailed scoring key for each of the variables is available here.
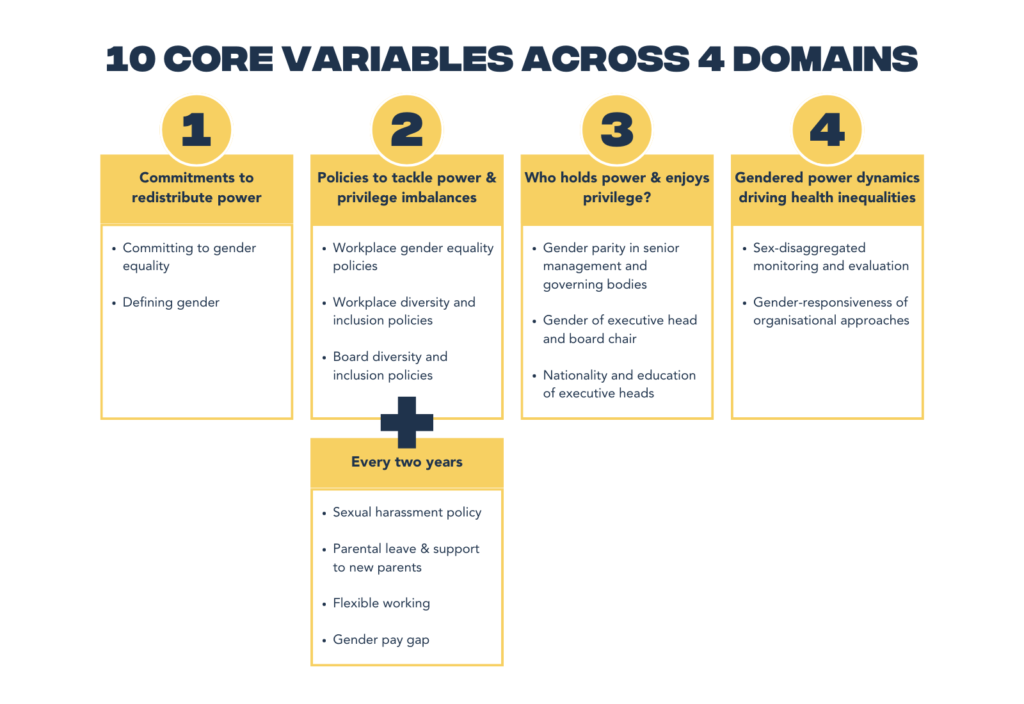
1) Commitment to redistribute power
Expand to read more
For long-term change to happen, it must be accompanied by change in discourse and narratives. The resurgence of a political backlash against the concept of ‘gender’ and the rise of interest groups who argue that gender is an “ideology”, or who deny that achieving gender equality includes realising sexual and reproductive health and rights for all, has made definitions and commitments more important than ever. Organisations must step up to define what they mean by gender and publicly commit to promoting equality as a core priority. There are two variables in this domain: committing to gender equality; defining gender.
2) Policies to tackle power & privilege imbalances at work
Expand to read more
To promote gender equality in health, organisations must first get their own houses in order. This means publishing policies which promote diversity and advance women’s careers, family-friendly workplaces that support caregivers and strive to achieve a work-life balance, and workplaces that are safe for all. There are three core variables in this domain: workplace gender equality policies; workplace diversity and inclusion policies; board diversity and inclusion policies. Every two years we conduct an in-depth review of the workplace policies and gender pay gaps of the organisation assessed in the report.
3) Equitable outcomes in power and pay/gender and geography of global health leadership
Expand to read more
Leadership which is diverse in gender and geography is key to achieving more supportive workplaces and more equitable health outcomes. Organisations need to support career progression, diverse hiring and appointment processes, and board diversity policies in order to ensure a gender balance in senior management, governing bodies and leadership, and a minimal gender pay gap. There are three variables in this domain: gender parity in senior management and governing bodies; gender of executive head and board chair; nationality and education of executive heads.
4) Addressing the gendered power dynamics of inequalities in health outcomes
Expand to read more
Gender affects the health of all people: men, women, non-binary and transgender populations. To address this, organisations and funders must put gender at the heart of their work by ensuring that their external policies, programmes and approaches (i.e. what they deliver) are fully gender-responsive. There are two variables in this domain: sex-disaggregated monitoring and evaluation; gender-responsiveness of organisational approaches.
Sampling and data collection on GH5050 ‘core variables’
To measure concepts as contextual as diversity and equality with a standardised, simple methodology may seem a fool’s errand. We recognise what has been called the ‘violence’ committed to nuanced concepts such as intersectionality when we attempt to reduce them to measurable indicators. Nonetheless, we are all aware that what gets measured, gets done.
Sample and criteria for inclusion
Expand to read more
The 2022 Report reviews 200 organisations active in global health. GH5050 defines “global organisations” as those with a presence in at least three countries. The sample includes organisations actively involved in global health and those organisations that aim to influence global health policy even if this is not their core function. Inclusion of an organisation does not signify GH5050’s endorsement of its activities, nor that GH5050 considers the organisation to be contributing to advancing population level health in a positive direction. Rather, organisations under review have been identified as having demonstrated an interest in influencing global health and/or global health policy.
Between 2018 and 2020, the sample shifted in its composition to account for 1) the thematic focus of the report each year, 2) continued efforts to identify global organisations headquartered in low- and middle-income countries, and 3) the general evolution of the global health architecture. Since 2020, the sample has not changed, except in the case of removing organisations that have ceased operations.
Ten sectors are represented in the 2022 sample:
- Public-private partnerships (PPPs), defined as those partnerships with for-profit and public sectors represented on their governing bodies (n=17);
- UN system agencies working in the health, nutrition and labour fields (n=11);
- Bilateral and global multilateral organisations, including the 10 largest bilateral contributors of development assistance for health in the period 2005-2015 (n=14);
- Funding bodies, including philanthropic organisations (n=14);
- Non-governmental and non-profit organisations, which can include industry groups registered as charitable organisations (e.g. 501(c)(3) in the US) (n=63);
- Private sector for-profit companies: Corporate participants in the Business and Health Action Group of the Global Business Council that provided a platform for the engagement of business in setting the health-related targets of the SDGs, or companies that contributed to consultations on the Uruguay Road Map on noncommunicable diseases (n=42);
- Consultancy firms with an interest in the health sector (n=10);
- Research and surveillance institutions (n=11);
- Faith-based organisations (n=10);
- Regional organisations (n=8).
We recognise the limitations of grouping organisations by sector, particularly in light of the unique features of many in our sample that preclude distinct categorisation. We have sought to establish clear rationale for the categorisation of each organisation, at times directly with the organisation.
Approach and methods for data collection
Expand to read more
GH5050 has developed a rigorous methodology that is consistent with established systematic review research methods. At least two reviewers extract each data item independently, and a third reviewer verifies the data. The reviewers discuss any discrepancies in data extraction until they reach a consensus. Data are coded according to content, using a traffic light system established in advance of data collection and refined iteratively. The codes in the GH5050 2022 report were updated from previous years, to bring further nuance and accuracy and as a result of invaluable ongoing discussions with organisations.
The data collected and analysed comes primarily from publicly-available websites. Transparency and accountability are closely related and by relying on publicly-available data we aim to hold organisations and stakeholders to account – including for having gender-related policies accessible to the public. We do not ask for confidential information, information of a commercially sensitive nature or information that would identify individuals in organisations (other than the gender of the CEO, for example, which is publicly available for all included organisations).
Several variables assess the availability and contents of policies. We do not consider newsletters or blogs as evidence of policy. Further, for workplace-related policies, we do not consider the contents of job advertisements as evidence of policy, Rather, we look for evidence of actual policies or an overall commitment from the organisation. This decision is also drawn from our concern that some people may not get as far as the job ads if they don’t see any commitment to equality in the main pages of the organisation itself.
Some organisations follow the workplace policies of host organisations or parent companies. In these cases, we used the same code as for the host/parent. For example, several organisations employ the workplace policies of the World Health Organization (WHO), e.g. Partnership for Maternal, Newborn and Child Health and the Alliance for Health Policy and Systems Research. Other non-workplace policy variables (e.g. gender parity in leadership, stated commitment to gender equality, etc.) are coded for each organisation individually.
For the corporate alliances and federations we looked for evidence of policies that were normatively gender equality-promoting. We did not accept evidence from members alone (e.g. IFBA has membership including Coca-Cola; we did not accept evidence of gender-responsive programmes from Coca-Cola for coding IFBA).
We used an earlier version of this methodology to review a small number of global health organisations and global PPPs in health. These reviews were published in peer-reviewed journals (The Lancet and Globalization and Health) prior to 2017.
Engaging and validating results with organisations
Expand to read more
We contact each organisation at least twice during the course of data verification. Initially we inform the CEO and head of human resources, or their equivalent, about the project and the start date of data collection, using email addresses found online. In that correspondence, we request the nomination and contact details of a focal point in the organisation who can review and validate the data once collected. Following completion of data collection, we send each organisation their preliminary results and ask them to review and provide any additional information, documentation or policies to review. In order to amend organisational scores, we request that organisations show us evidence in the public domain to support their amendment. Throughout the process of data collection, GH5050 encourages organisations to contact us to discuss queries about the process and the variables. Final results are shared with all organisations before publication.
Ethics
The methods described above have been approved by the ethics committee of University College London, where GH5050 was previously housed.
Strengths and limitations
Expand to read more
As far as we know, this is the only systematic attempt to assess how gender is understood and practised by organisations working in and/or influencing the field of global health across multiple dimensions (commitment, workplace policy content, gender and geography of leadership and gender-responsive programming). While our efforts may have omitted relevant measures and do not include all active organisations, this method provides the opportunity to measure status quo and report on organisations’ progress. This method has allowed us to shine a light on the state of gender equality in global health and organisations across all sectors have begun to respond to our call. We believe that the collection of data and information for measurement and accountability is a fundamental first step to change.
Last updated 13 January 2023.
