
What insights can sex-disaggregated data offer—and how can it help inform national and international responses to the pandemic?
Re-posted from ICRW. This month, ICRW Asia—in partnership with Global Health 50/50 and the African Population and Health Research Center (APHRC)—launched the world’s largest and most comprehensive sex-disaggregated COVID-19 database. Dr. Ravi Verma, Director of ICRW Asia and an advisor for the partnership, discusses what insights the data has to offer—and how it can help inform national and international responses to the pandemic.
What is the partnership seeking to achieve?
Ravi: This partnership is a unique attempt to understand how COVID-19 is impacting people differently due to sex and gender—both in terms of biology as well as the social environment, structures and norms—and to produce the data needed for truly gender-responsive approaches to the pandemic.
Global Health 50/50’s international framework, combined with regional and country-specific perspectives from ICRW Asia and APHRC, allows us to create a more comprehensive body of evidence on the extent to which countries are gathering this data and making it public. The resulting database allows us to better advocate for more consistent and credible data, and to provide insights for countries to respond to the unique segments of their population.
What does the tracker reveal about the gender-related impacts of COVID-19?
Ravi: Tracking over 170 countries across the world, the dashboard represents the first systematic data-gathering process to understand how men and women are being differentially impacted by COVID-19. Overall, while cases are evenly reported among both men and women, men account for 40 percent more COVID-19 deaths. Gendered differences exist along the clinical pathway, from testing through to intensive care admissions.
However, fewer than one in three of the world’s countries are reporting sex-disaggregated data for both COVID-19 cases and deaths; among the 173 countries currently tracked, 75 reported no data separately for women and men in the last month.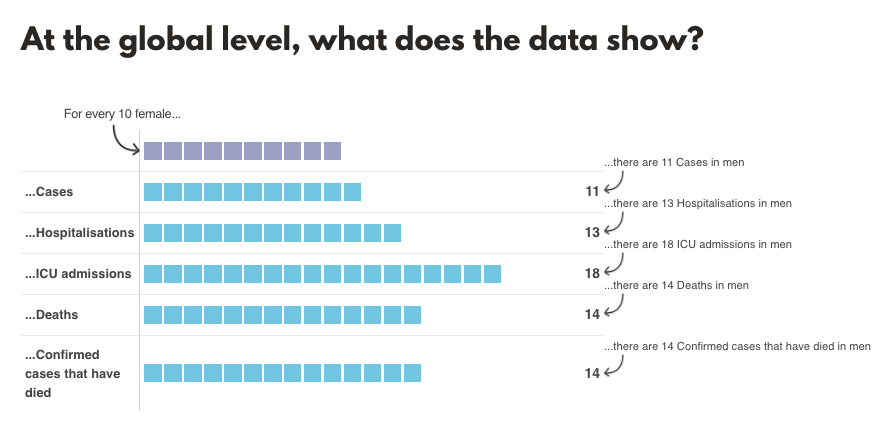
How is this data relevant at the country level, in India in particular?
Ravi: Unequal gender norms are deeply entrenched in Indian society and mindsets. We also know that women and men face differential exposure to risk given the expectations and perceptions around what women and men should be doing.
However, India is one country that does not systematically release sex-disaggregated data at the state or national level, and our data is also limited and inconsistent in terms of how it represents different aspects of the pandemic. So this effort to systematically gather the data would provide a deeper insight into how gender norms relate to other systemic inequalities—such as caste and class—and how interventions can address the intersectional nature of the risks and vulnerabilities with respect to COVID-19.
What are the next steps for the partnership?
Ravi: It’s critical to think about both short-term and long-term implications. In the short term, we hope the data generated by this project will help inform policymaking, and in the medium term, that it will also help program personnel create gender-responsive strategies in their countries to reach the most vulnerable.
In the long term, we hope to provide an evidence-based, gender-responsive public health model. In order to keep building toward a more comprehensive body of evidence, we are urging governments to make a commitment to collect data—by both sex and gender—and make that data available to the wider community of practice.
Find out more about the Sex, Gender and COVID-19 Project and explore the Tracker.
 As Director of ICRW Asia, located in New Delhi, India, Dr. Ravi Verma leads ICRW’s local and regional efforts to conduct research, provide technical support, build capacity and partake in policy dialogue on an array of issues, including reproductive health, family planning, preventing domestic violence, child marriage, engaging men and boys to empower women, HIV/AIDS and economic development.
As Director of ICRW Asia, located in New Delhi, India, Dr. Ravi Verma leads ICRW’s local and regional efforts to conduct research, provide technical support, build capacity and partake in policy dialogue on an array of issues, including reproductive health, family planning, preventing domestic violence, child marriage, engaging men and boys to empower women, HIV/AIDS and economic development.
