This past year the term ‘sex-disaggregated data’ may, for the first time, have become part of common parlance. The COVID-19 pandemic has driven an influx of interest in the role sex and gender as drivers of health outcomes. COVID-19 is not an exception; across all areas of health, differences in exposure and outcomes are driven by sex and gender. Sex-disaggregated data, combined with gender analysis, contributes to identifying health disparities, shaping programmes to address them and measuring whether such programmes are reaching different populations equitably. Sex-disaggregation (along with age-disaggregation) of data should be ubiquitous within health programmes: it is a means to hold organisations to account for their commitments not only to equity but also to the delivery of effective interventions.
“Without informed responses from leaders, we are going to perpetuate inequities. But the good news is that this is a preventable problem - we have the tools, we have the knowledge, we have the skills. Now we have to make sure we have the resources and the motivation to change this.”
Emily Courey Pryor, Executive Director, Data2x
Findings
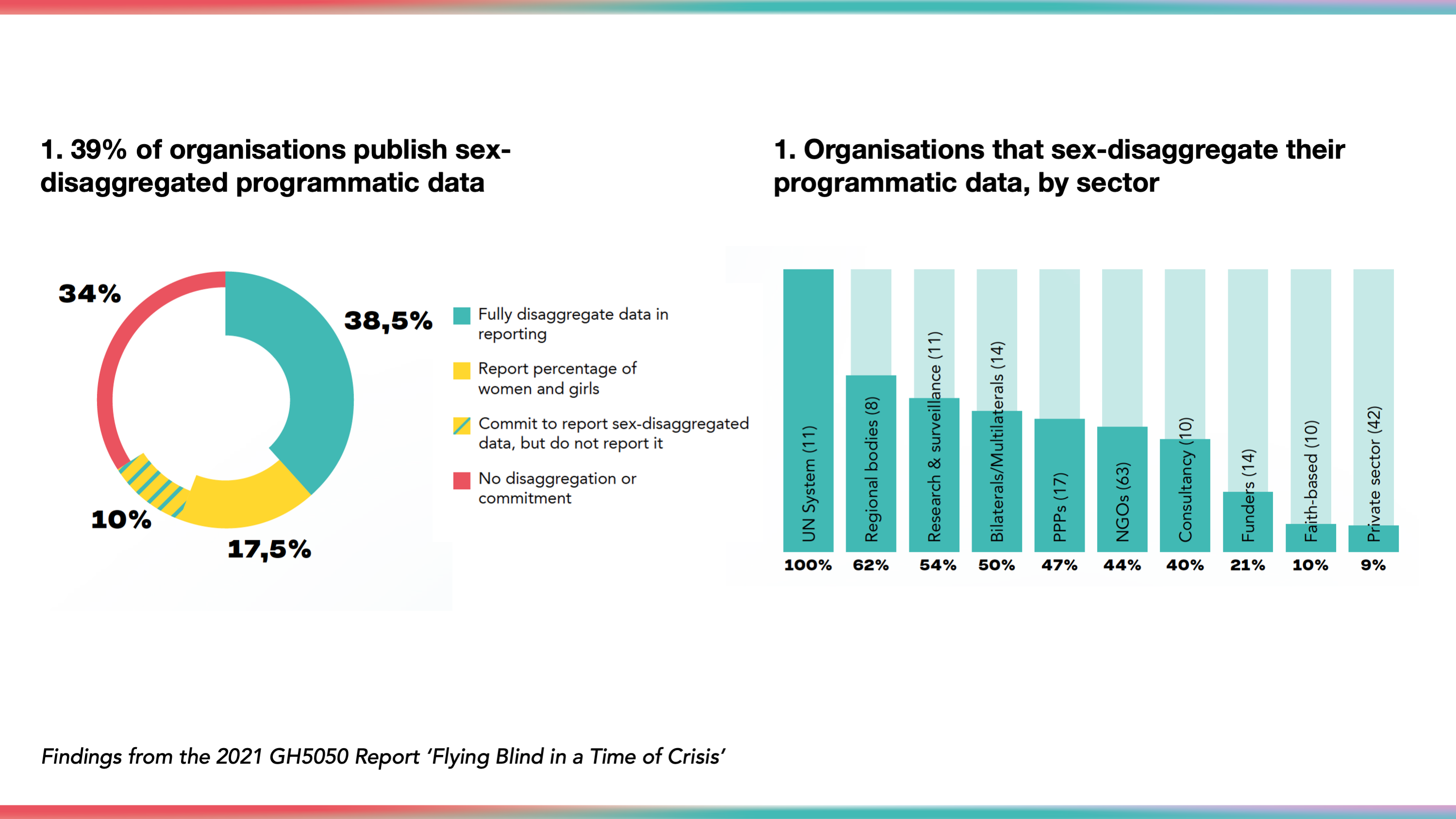
39% of organisations were found to be providing data on their programmatic delivery broken down by sex. A further 28% of organisations report on the proportion of beneficiaries who are women and girls. For 34% of organisations, no sex-dissggregation of data was found.
Among the 139 organisations reviewed consistently from 2018 to 2021, reporting of sex-disaggregated data has barely budged, shifting from 35% in 2018 to 36% in 2021.
“Am I surprised that fewer than the GH5050 report finds just 4 in 10 organisations publish sex-disaggregated data? Sadly, no I’m not. But lives have been saved because of sex-disaggregating data. Humans are not unisex, so it doesn’t make sense to treat data that way.”
Caroline Criado-Perez, author of Invisible Women